(NEW!) CLINICAL TRIALS IN THE ICU

CLINICAL TRIALS IN THE ICU
TUESDAY OCTOBER 23RD
![]() #LIVES2018
#LIVES2018
This session featuring results from some of the newest clinical trials – all published in Intensive Care Medicine is led by ICM Editor-in-Chief Elie Azoulay (Paris, France) and Maurizio Cecconi (Milan, Italy). Of course, this ground-breaking session is not just about presentation of clinical trial results… each presentation has an appointed commentator to discuss strengths and limitations of the trial and a discussion period, so delegates can ask questions as well!
Watch the full session here!
Scroll down to the full list of presentations for links to the articles published simultaneously in Intensive Care Medicine and interviews with some of the study authors.
Featured presentations:
L/KG/MIN: More efficient than 2 L/KG/MIN to support young infants with severe viral bronchiolitis
using high-flow nasal cannulae? Multicentre randomised controlled trial (TRAMONTANE 2 Study)
This RCT compared two flow rates for nasal cannula therapy in viral bronchiolitis.
We found that using HFNC with a flow setting of 3 L/kg/min did not reduce the risk of failure in young infants with acute viral bronchiolitis. A flow rate of 2 L/kg/min, associated with less discomfort and shorter stay in the PICU, should be favored for clinical practice.
~ Christophe Milesi
A multicentre randomised pilot trial on the effectiveness of different levels of cooling in comatose survivors of out-of-hospital cardiac arrest: The FROST-I trial
The results of this study do not allow us to establish an optimum level of TTM to be applied to comatose survivors of OHCA. However, although no differences or trends were observed between study groups, it cannot be definitively concluded that all three-temperature levels are equally effective. Among patients who died, there was a significant trend of lower withholding life sustaining therapies because of severe brain damage with lower temperatures.
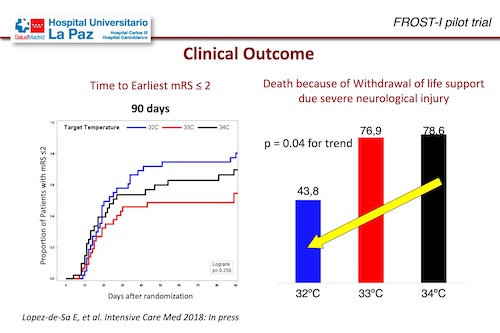
 Information about TTM at 32ºC is scarce. With this study now we know that comatose resuscitated OHCA patients after shockable rhythms can be managed at a TTM of 32°C in a fast, accurate and precise manner, with intravascular cooling. The use of lower target temperatures seems to be safe, does not increase the rate of infection, although there is a further decrease in heart rate. Future research should explore efficacy of 32ºC target and should also analyse isolated neurological endpoints where TTM seems to be more effective.
Information about TTM at 32ºC is scarce. With this study now we know that comatose resuscitated OHCA patients after shockable rhythms can be managed at a TTM of 32°C in a fast, accurate and precise manner, with intravascular cooling. The use of lower target temperatures seems to be safe, does not increase the rate of infection, although there is a further decrease in heart rate. Future research should explore efficacy of 32ºC target and should also analyse isolated neurological endpoints where TTM seems to be more effective.
~ Esteban Lopez-de-Sa
Want to read more great new articles?To access more articles on the ICM website, click here.
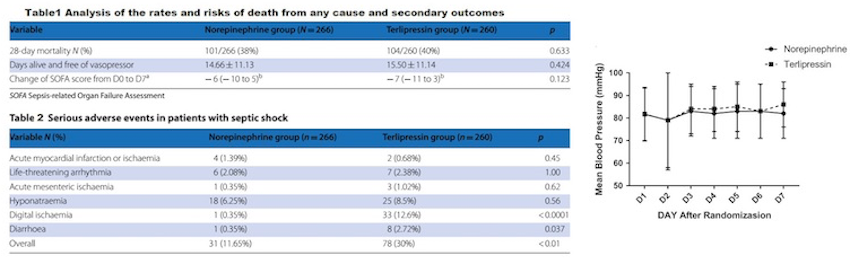
 Terlipressin versus norepinephrine as infusion in patients with septic shock: A multicentre, randomised, double-blinded trial
Terlipressin versus norepinephrine as infusion in patients with septic shock: A multicentre, randomised, double-blinded trial
This is the largest randomised, controlled, double-blind multicentre study comparing terlipressin and norepinephrine conducted to date. Continuous administration of terlipressin compared to NE in patients with septic shock, did not decrease 28-day mortality. The changes in SOFA score on day 7 after randomisation were similar in the two groups. Terlipressin might be an alternative vasopressor in septic shock. Digital ischaemia should be closely monitored during terlipressin infusion.
This trial raises some questions such as:
1. The indications for the infusion of terlipressin in septic shock
2. What might be the suitable dosage of terlipressin in septic shock?
3. The effect of terlipressin on renal function
~ Guan Xiangdong
Plasma angiopoietin-2 as a potential causal marker in sepsis-associated ARDS development:  Evidence from mendelian randomisation and mediation analysis
Evidence from mendelian randomisation and mediation analysis
Using the genetic technique Mendelian Randomisation Analysis, we used genetic variation as an instrumental variable to predict plasma angiopoietin-2 in patients with sepsis. This technique uses the principle of random assortment of genotypes at gametogenesis to infer the causality of a marker on a disease. In our study, the genetically predicted plasma angiopoietin-2 was associated with ARDS risk in sepsis, inferring plasma angiopietin-2 may play a causal role in ARDS development. Strategies to reduce plasma angiopoeitin-2 warrant prioritisation for testing to prevent or treat sepsis-associated ARDS.
~ John P. Reilly
Small volume resuscitation with 20% albumin in intensive care: Physiological effects 
In haemodynamically unstable ICU patients, what is the feasibility and efficacy of small volume resuscitation with 20% albumin as opposed to resuscitation with 4-5% albumin?
The SWIPE trial, an open label, multicentre, randomised controlled trial demonstrates that small volume resuscitation with 20% albumin reduced resuscitation fluid requirements and minimised fluid accumulation compared with resuscitation with 4-5% albumin. Despite lower resuscitation volumes, small volume resuscitation with 20% albumin produced a similar early haemodynamic
response as larger volume resuscitation with 4-5% albumin.
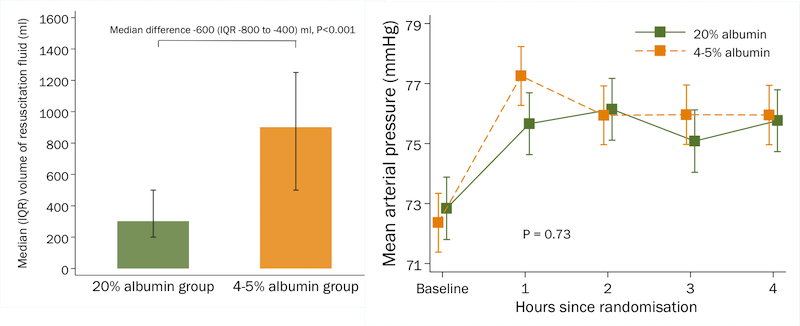
Small volume resuscitation with 20% albumin produced a similar haemodynamic response as larger volume resuscitation with 4-5% albumin
~ Johan Mårtensson
 Impact of a multifaceted prevention programme on ventilator-associated pneumonia including selective oropharyngeal decontamination
Impact of a multifaceted prevention programme on ventilator-associated pneumonia including selective oropharyngeal decontamination
The implementation of a multifaceted programme consisting in 9 preventive measures, including selective oropharygeal decontamination was able to dramatically decrease the incidence of VAP in a polyvalent Swiss ICU.
~ Jérome Pugin
>> Find the full list of clinical trial presentations and commentators with relevant links here:
L/KG/MIN: More efficient than 2 L/KG/MIN to support young infants with severe viral bronchiolitis using high-flow nasal cannulae? Multicentre randomised controlled trial (TRAMONTANE 2 Study)
Speaker: Christophe Milesi, Montpellier, France
Commentator: Miet Schetz, Leuven, Belgium
A multicentre randomised pilot trial on the effectiveness of different levels of cooling in comatose survivors of out-of-hospital cardiac arrest: The FROST-I trial
Speaker: Esteban Lopez-de-Sa, Madrid, Spain
Commentator: Giuseppe Citerio, Monza, Italy
Terlipressin versus norepinephrine as infusion in patients with septic shock: A multicentre, randomised, double-blinded trial
Speaker: Guan Xiangdong, Guangzhou, China
Commentator: Ignacio Martin-Loeches, Dublin, Ireland
LINK TO PAPER: Original ~ Terlipressin versus norepinephrine as infusion in patients with septic shock: a multicentre, randomised, double-blinded trial (icTV interview with presenting author will be online soon!)
Plasma angiopoietin-2 as a potential causal marker in sepsis-associated ARDS development: Evidence from mendelian randomisation and mediation analysis
Speaker: John P Reilly, Philadelphia, United States
Commentator: Laurent Papazian, Marseille, France
Small volume resuscitation with 20% albumin in intensive care: Physiological effects
Speaker: Johan Mårtensson, Stockholm, Sweden
Commentator: Anders Perner, Copenhagen, Denmark
Questions to improve family-staff communication in the ICU: A randomised controlled trial
Speaker: Elie Azoulay, Paris, France
Commentator: Giuseppe Citerio, Monza, Italy
Impact of a multifaceted prevention programme on ventilator-associated pneumonia including selective oropharyngeal decontamination
Speaker: Jérome Pugin, Geneva, Switzerland
Commentator: Laurent Papazian, Marseille, France
Safety and tolerability of a single administration of AR-301, a human monoclonal antibody, in ICU patients with severe pneumonia caused by Staphylococcus aureus: First-in-human trial
Speaker: Pierre-François Laterre, Louvain, Belgium
Commentator: Samir Jaber, Montpellier, France
Thematic Session ~ CLINICAL TRIALS IN THE ICU
23.10.2018, 16:00 – 18:08, Room Paris