New Publication | Clinical criteria for the definition of refractory septic shock: a joint Delphi consensus from the Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM)
Refractory septic shock finally has a definition: a major step forward for intensive care. For the first time, an international expert panel assembled by SCCM and ESICM has reached consensus on structured clinical criteria to define refractory septic shock — one of the most severe and poorly characterised conditions in intensive care medicine.
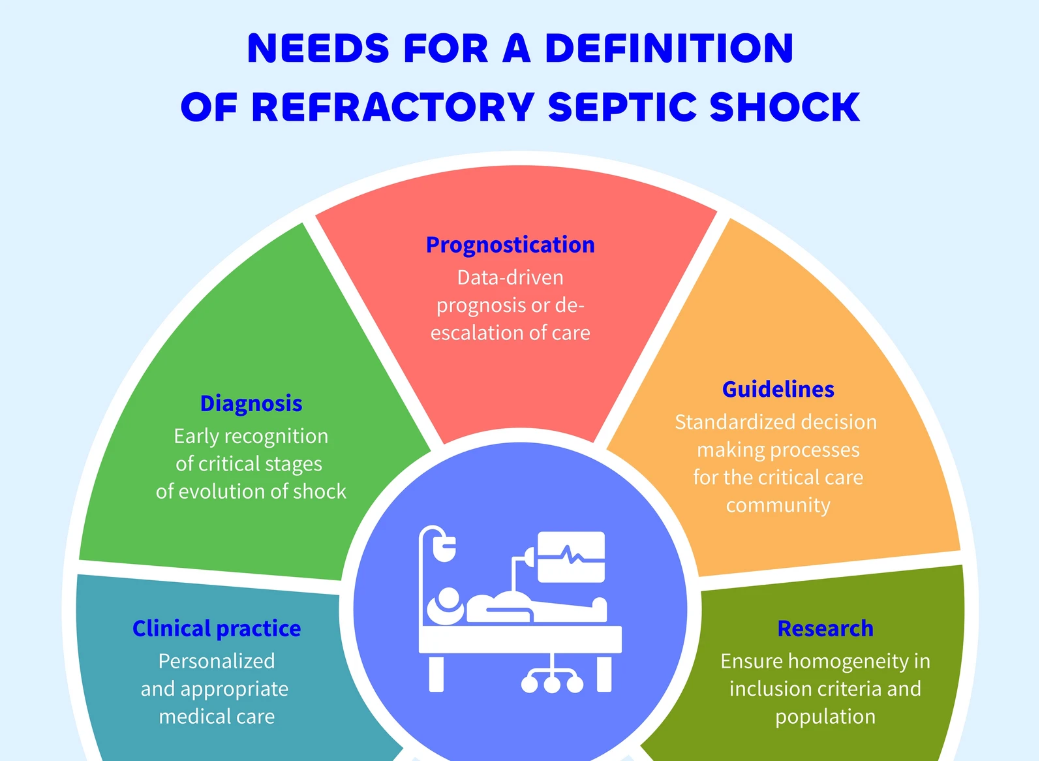
Despite being widely used in clinical trials, research, and scientific meetings, the term “refractory septic shock” has long suffered from a striking paradox: no formal, robust definition existed. A systematic review of the literature revealed marked variability in how the term was applied — with inconsistent thresholds for hypotension, hyperlactatemia, and vasopressor doses across studies — undermining comparability, weakening clinical guidance, and leaving the most critically ill patients without a standardised framework for diagnosis and management.
To address this gap, ESICM and SCCM convened a diverse panel of 56 multinational, multiprofessional experts from 22 countries across five continents, including intensivists, nurses, pharmacists, and a PhD scientist, co-chaired by Ashish Khanna and Marc Leone. Through a rigorous five-round Delphi process conducted between May and September 2025, the panel evaluated 34 statements across eight clinical domains. Consensus was reached on 13 key criteria, culminating in a clear, bedside-applicable definition:
Refractory septic shock is defined as the presence of persistently elevated lactate concentrations and/or prolonged capillary refill time in a patient with septic shock who is fluid unresponsive, requiring a norepinephrine equivalent dose greater than 0.5 µg/kg/min, with confirmation by intensive care ultrasound (CCUS) when mixed shock is suspected.
Critically, CCUS was the only diagnostic modality to achieve strong consensus agreement (92.9%), reflecting the central role of bedside ultrasound in modern shock management. The framework is intentionally aligned with the existing Sepsis-3 definitions and Surviving Sepsis Campaign guidelines, positioning it as a practical clinical tool rather than an academic exercise.
The authors acknowledge that these criteria require external validation before clinical adoption or inclusion in future guidelines — but the establishment of a common language marks a decisive turning point. It enables better phenotyping of the most severe septic shock patients, supports the design of more targeted clinical trials, and opens the door to precision medicine approaches in this high-mortality population.